Deciphering the Complex Etiology of Type 1 Diabetes
Published on 12 Apr, 2024

Type 1 diabetes (T1D) is a complex autoimmune disease with a multifactorial etiology. Genetic predisposition, environmental triggers, and immune dysregulation contribute to the development of this chronic condition. Diagnoses involves a combination of clinical evaluation, laboratory tests, and medical history assessment. T1D impacts millions globally, with its incidence rising notably among African American and Hispanic youth populations. A variety of treatment options, including maintenance therapy, transplants, gene therapy, vaccines, antibodies, and combination therapies, are being explored to improve outcomes and quality of life for individuals with T1D.
Type 1 diabetes is a chronic autoimmune disorder characterized by the destruction of insulin-producing beta cells in the pancreas. It affects millions worldwide, with onset typically occurring during childhood or adolescence. While the precise cause remains elusive, extensive research has uncovered key insights into its etiology.
Etiology of Type 1 Diabetes
- Genetic Predisposition: Genetic predisposition refers to an individual's inherent susceptibility or increased likelihood of developing a particular trait or condition due to variations in their genetic makeup. These predispositions may arise from specific gene mutations, allelic variations, or genetic polymorphisms that can influence an individual's response to environmental factors or their risk of developing certain diseases.
- HLA Genes: The HLA region on chromosome is a critical susceptibility locus for T1D. HLA genes exhibit numerous variations, forming unique combinations called haplotypes. Certain haplotypes, especially those of HLA-DQA1, HLA-DRB1, and HLA-DQB1 gene variations, heighten T1D risk of an exaggerated immune response to beta cells, contributing about 40% to T1D's genetic risk.
- Rare Monogenic Forms: Rarely, autoimmune diabetes stems from mutations in a single gene, leading to monogenic forms often linked to other autoimmune conditions due to shared regulatory pathways. One example is the IPEX syndrome (Immune dysregulation, polyendocrinopathy, enteropathy, X-linked), caused by Foxp3 transcription factor mutations, disrupting Treg function and prompting multiorgan autoimmunity. Approximately 80% of affected children develop T1D.
- Insulin Gene: The IDDM2 locus on chromosome 11, containing the insulin gene region, confers a minor genetic predisposition to T1D. Variations in the variable number of tandem repeat (VNTR) polymorphisms in the insulin gene's promoter region determine susceptibility, with shorter repeats (VNTR type I) increasing risk and longer repeats (VNTR type III) offering protection against T1D.
- PTPN22: A relatively new addition to the T1D susceptibility gene set is PTPN22, which encodes for the lymphoid protein tyrosine phosphatase (LYP). A mutation resulting in loss of function can lower the threshold for autoreactive T-cell activation.
- IL2RA: Allelic variations in IL2RA are strongly linked to T1D susceptibility. Detected Single nucleotide polymorphisms (SNPs) in the IL2RA gene from genome-wide studies suggest increased T1D risk by affecting IL2RA expression or function, thereby altering Treg function and immune regulation.
- CTLA-4: CTLA-4 regulates T-cell activation and enhances regulatory T-cell function, influencing immune tolerance. Genetic variations in CTLA4 are associated with T1D susceptibility. Therapeutic strategies targeting CTLA-4 signaling hold promise for T1D treatment by modulating immune responses and restoring tolerance.
- Precipitating Events: Autoimmunity is considered to be the predominant effector mechanism of T1D; however, it may not be its primary trigger. T1D precipitates in genetically susceptible individuals, often triggered by environmental factors. However, there remains a significant gap between the initiation and detection of ongoing diabetogenic incidents, posing a fundamental challenge in identifying potential causative environmental triggers. Some of the plausible environmental triggers include:
- Enteroviruses: Enteroviruses, particularly Coxsackie virus B, are implicated in triggering autoimmune responses causing T1D. These infect pancreatic beta cells, inducing inflammation and disruption immune tolerance mechanisms, advancing T1D in genetically predisposed individuals.
- Bacteria: The gut microbiota, especially the bacterial composition (lipopolysaccharide content), correlates with T1D prevalence. Butyrate-producing bacteria levels are associated with autoantibodies, suggesting a potential preventive strategy. Moreover, gut virome and mycobiome variations may impact immune dysregulation and T1D development.
- Other Environmental Triggers: Cow milk and wheat proteins have shown conflicting associations with T1D, especially in early childhood exposure. Vitamin D shows protective effects, with lower levels linked to increased risk due to its role in immune regulation and maintaining self-tolerance.
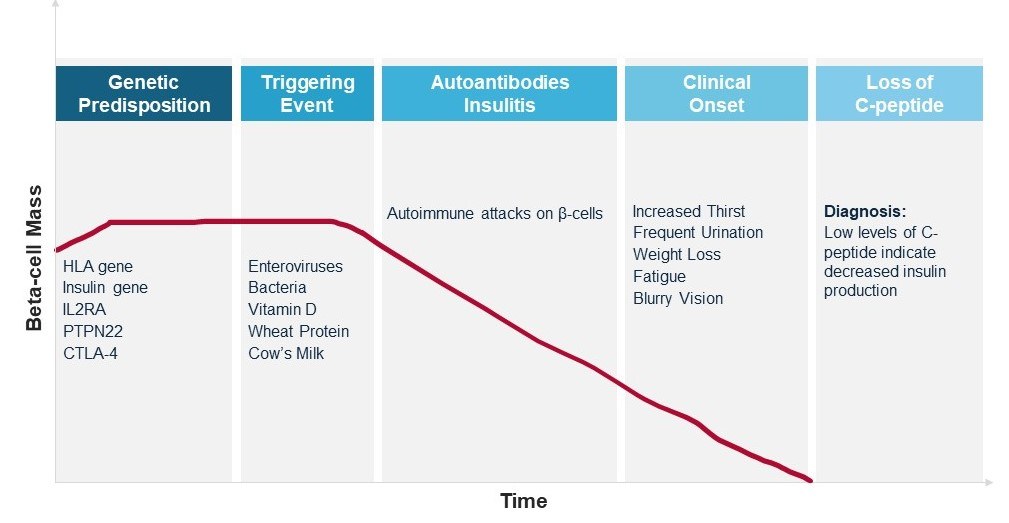
Figure 1 - Type 1 Diabetes Development and Progression
Diagnosis
Diagnosing T1D entails clinical evaluation, lab tests, and a review of medical history. Some of the techniques involved include symptom assessment, blood glucose measurement, and autoantibody testing. Biomarkers such as islet autoantibodies (e.g., GAD, IA-2, ZnT8), C-peptide levels, and glycated hemoglobin (HbA1c) help gauge the risk of clinical diagnosis. These biomarkers provide insights into the autoimmune destruction of pancreatic beta cells and are utilized as prognostic biomarkers to monitor the rate of disease progression.
Prevalence of Type 1 Diabetes
According to a research article published in the Lancet (2022), T1D affected 8.4 million individuals globally in 2021, with 1.5 million (18%) below 20 years, 5.4 million (64%) aged 20–59, and 1.6 million (19%) aged 60 or older. Approximately 0.5 million new cases emerged, with a median onset at 29 years, and around 35,000 non-diagnosed deaths within a year. Additionally, 1.8 million individuals lived in low-income settings. Projections suggest that by 2040, cases may rise to 13.5–17.4 million, particularly in low-income countries.
Another review published in Plos Global Public Health in 2022 found that the highest T1D incidence rates were reported in the 5–9 and 10–14-year age groups than in the 0–4 and 15–19 year age groups. Moreover, in the 0–14-year age group, the highest incidence was reported in Northern Europe (23.96 per 100,000), Australia/New Zealand (22.8 per 100,000), and Northern America (18.02 per 100,000), while the lowest was observed in Melanesia, Western Africa, and South America (all <1 per 100,000).
Treatment
T1D treatments encompass a range of diverse strategies aimed at managing blood sugar levels and preventing complications. These include maintenance therapy, which comprises numerous strategies such as insulin therapy with various formulations and delivery methods, and pancreas or islet cell transplantation, which is tailored to individual needs to ensure optimal glycemic control and long-term management of the condition. However, more advanced therapies such as gene therapy aim to restore beta cell function, while immunomodulatory vaccines and monoclonal antibodies target immune responses. Combination therapies, such as insulin paired with immunomodulatory drugs or stem cell transplantation, offer synergistic approaches to manage T1D, addressing both glycemic control and immune regulation for enhanced treatment efficacy and patient well-being.
Future Perspective
Recent research has focused on identifying biomarkers for early detection of and intervention in T1D. Advances in genetic sequencing technologies have aided the identification of novel susceptibility loci and pathways involved in disease pathogenesis. Immunomodulatory therapies focused on preserving beta cell function and inducing immune tolerance show promise in preventing or delaying the onset of T1D in at-risk individuals.

Aditi Thakur
